

INTRODUCTION
Older AML patients have a different mutational landscape compared to younger patients. The prognostic classification of AML proposed by the European Leukemia Net (2017) is based on the presence of mutations in FLT3 (ITD), NPM1, CEBPA, RUNX1, ASXL1 and TP53. However, our group has identified a high-risk prognostic score in older patients with AML, who are undergoing treatment with azacitidine or low-dose cytarabine plus fludarabine, which predict a shorter survival.
OBJECTIVE
Validation of the previously identified high-risk prognostic score, defined by the presence of mutations in NRAS or TP53, in 3 cohorts of patients with AML who have been studied by NGS with a custom panel in the healthcare practice (Cohort 1: Intensive treatment; cohort 2: Hypomethylating agents and cohort 3: low-dose cytarabine)
METHODS
The study was conducted on a series of 535 patients diagnosed with AML (mean age 67). Patients evaluated for OS and RFS were 497 cases: intensive treatment (schemes 3+7 or similar; n=238), hypomethylating agents (azacitidine, decitabine; n=113) and treated with low-dose cytarabine (n=146). 38 patients on supportive therapy were excluded.
Mutational profile was identified at diagnosis by NGS technique (Ion Torrent System), using a custom panel of 41 genes involved in myeloid pathologies: ASXL1, BCOR, BCORL1, CALR, CBL, CEBPA, DNMT3A, EPAS1, EPOR, ETV6, EZH2, FLT3, IDH1, IDH2, JAK2, KDM6A, KIT, KMT2A, KRAS, MPL, NF1, NPM1, NRAS, PHF6, PRPF40B, RAD21, RUNX1, SETBP1, SF3A1, SF3B1, SH2B3, SMC1A, SRSF2, STAG2, TET2, THPO, TP53, U2AF1, VHL, WT1 y ZRSR2.
The mean OS and RFS were compared by means of Kaplan-Meier curves using the log-rank test. The bioinformatics analysis was performed with the SPSS software.
RESULTS
The median SG and RFS of this series was 10.8 months and 6.9 months respectively.
The mutational profile in older patients was different from that analyzed in younger patients. We observed greater presence of mutations in NPM1 in younger patients (34.4 vs 18.6%, p=0.04), while in older than 65 years were identified more mutations in ASXL1 (3.9 vs 16.6%, p<0.01) or RUNX1 (8.6 vs 18.4%, p=0.005). No differences were observed in TP53, NRAS, TET2, DNMT3A and FLT3-ITD. However, we detected differences in VAF distribution of variants with lower VAF in younger patients in NPM1 (0.9 vs 5%, p=0.001), RUNX1 (4.1 vs 9.1%, p=0.003), ASXL1 (1.5 vs 8.2%, p<0.001) and TP53 (5.9 vs 14%, p<0.001)
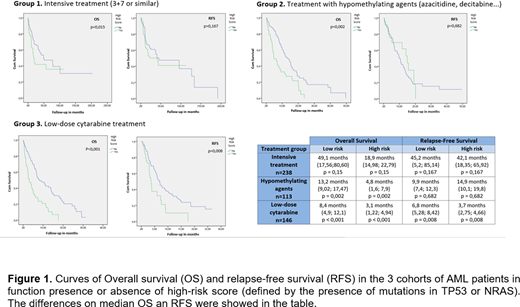
The median OS for intensively treated patients with a low-risk prognostic score was 49.1 months (17.56, 80.60) vs. 18.9 (14.98, 22.79) for high-risk patients (p=0.015). The median RFS was 45.2 months (5.2; 85.14) for low-risk patients vs. 42.1 (18.35; 65.92) for high-risk patients (p=0.167).
The median OS for low-risk patients treated with hypomethylating agents was 13.2 months (9.02, 17.47) vs. 4.8 (1.6, 7.9) for patients with a high-risk score (p=0.002). The median RFS was 9.9 months (7.4, 12.3) for low-risk patients vs. 14.9 (10.1, 19.8) for high-risk patients (p=0.682).
The median OS for patients treated with low-dose cytarabine was 8.4 months (4.9, 12.1) for low risk vs. 3.1 (1.22, 4.94) for high risk (p<0.001). The median RFS was 6.8 months (5.28, 8.42) for low-risk patients vs. 3.7 (2.75, 4.66) for those with a high-risk score (p=0.008).
CONCLUSIONS
We have confirm that exist differences in the mutational profile between older and younger AML patients and these differences have implications in the definition of risk of these patients. The prognostic score defined by the presence of mutations in the TP53 and NRAS genes, has been validated as an adverse prognostic factor across the three treatment groups studied (intensive treatment, hypomethylating agents and low-dose cytarabine) for OS, and this score no predict risk of relapse in the cohorts with intensive and hypomethylating treatments at difference to the low-dose cytarabine cohort.
ML.M. enjoys a research grant from the Spanish Society of Hematology and Hemotherapy. This work has been financed thanks to the aid PI16/01225 and PI19/01518, from the Instituto de Salud Carlos III (Ministerio de Economía, Industria y Competitividad) and co-financed by the European Development Fund.
Montesinos:Astellas, Novartis, Janssen: Speakers Bureau; Celgene, Pfizer, Abbvie: Consultancy; Pfizer, Abbvie, Daiichi Sankyo: Research Funding. Martinez-Lopez:Incyte: Consultancy, Research Funding; Janssen: Consultancy, Honoraria; Janssen-cilag: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Novartis: Consultancy; BMS: Consultancy, Research Funding. Sanz:Teva, Daiichi-Sankyo, Orsenix, AbbVie, Novartis, and Pfizer: Other: Consulting or Advisory Role.

